Skin Cancer surgery
In our world, this suture job is unacceptable. The sutures are too big. The edges are rolled in. The patient was told to return in ten days, at which time the suture tracts will epithelialize, resulting in Frankenstein railroad tracts.
SECRET: Insurance companies will pay the exact same amount for a skin cancer to be removed by a highly skilled plastic surgeon, as they will for a dermatologist, nurse, or technician! There is no dermatologist, nurse, or technician on the planet with the skills of a board certified plastic surgeon with five years of surgical training and reconstructive plastic surgery residency. In my humble opinion. 🤔🤫
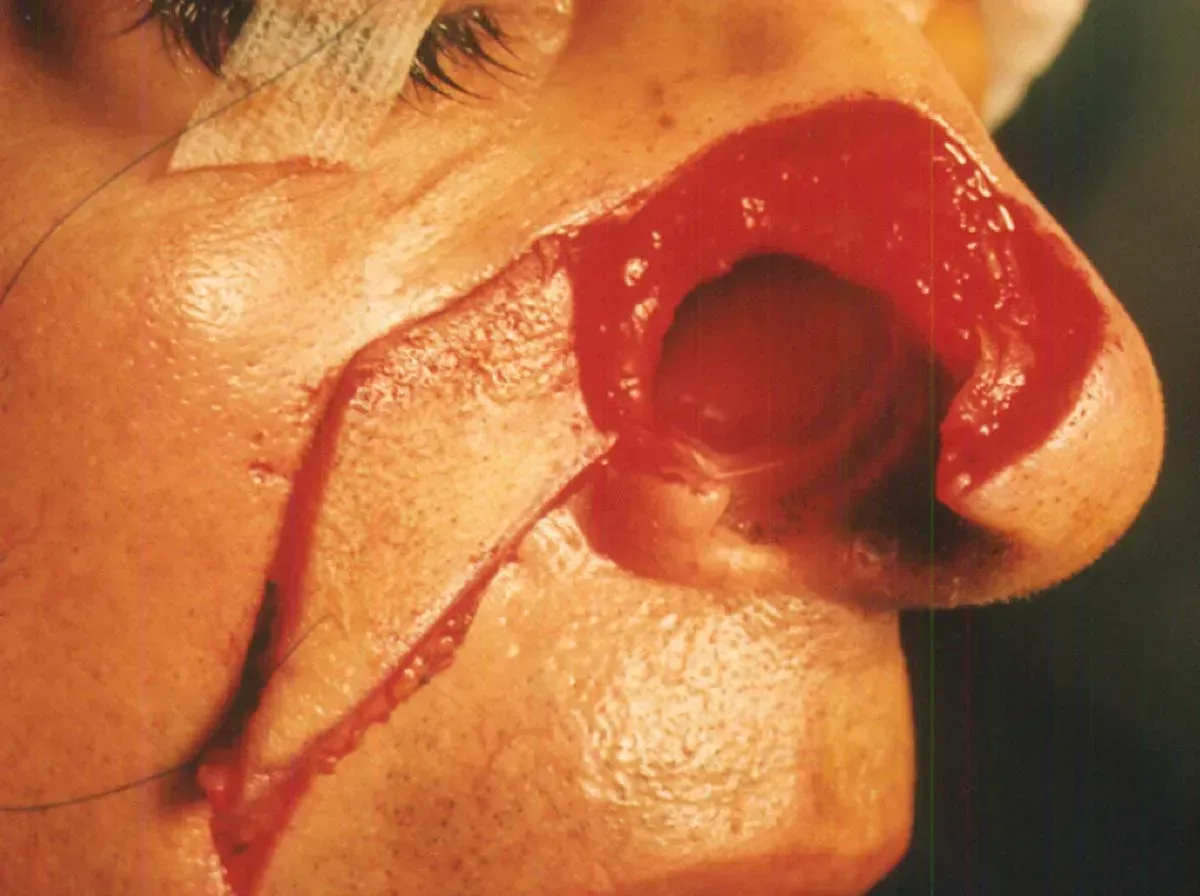
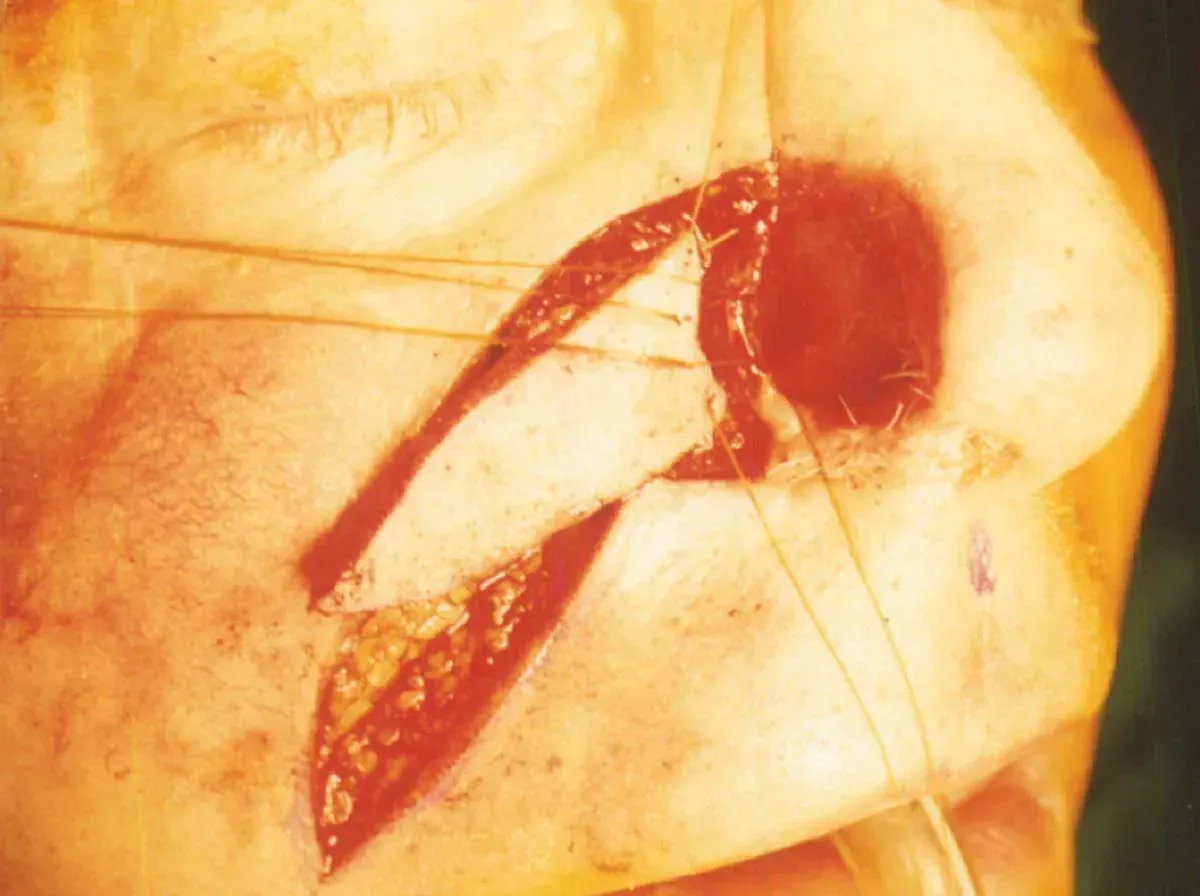
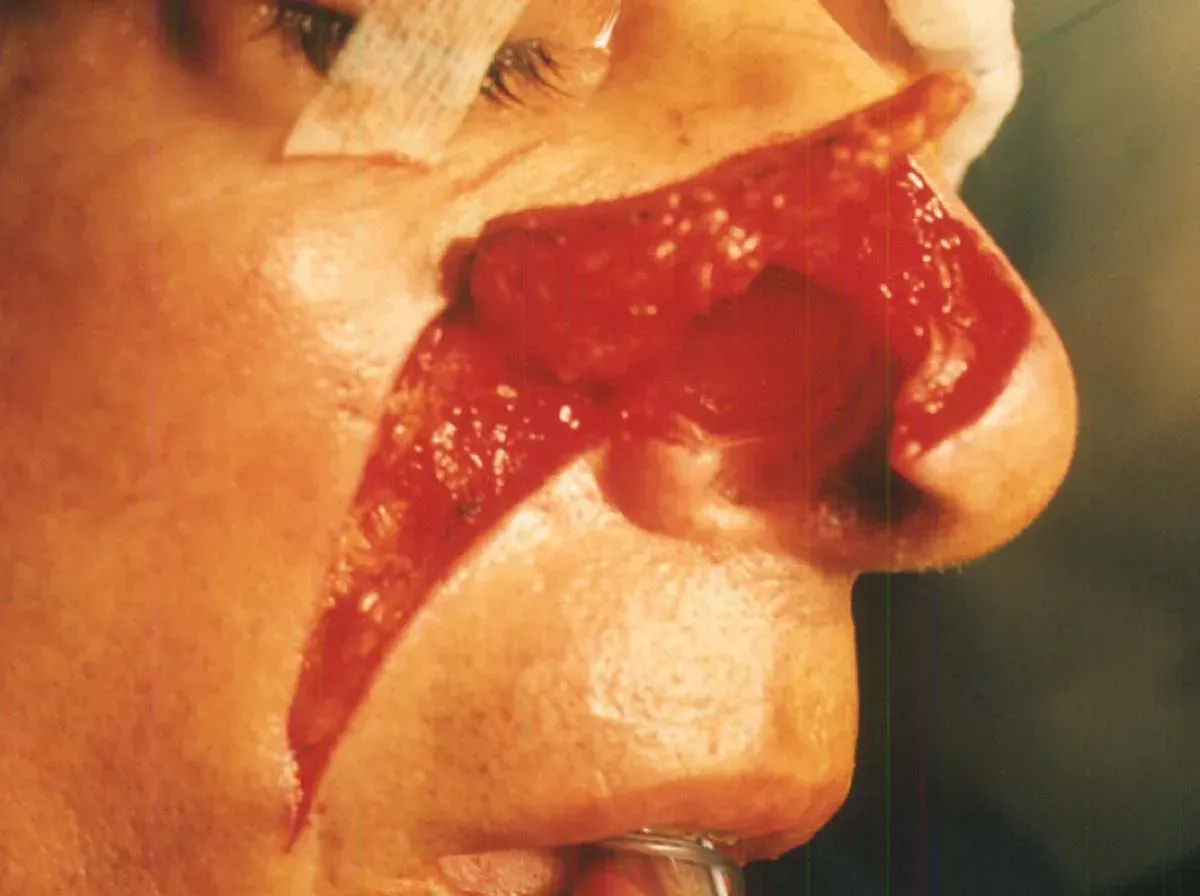
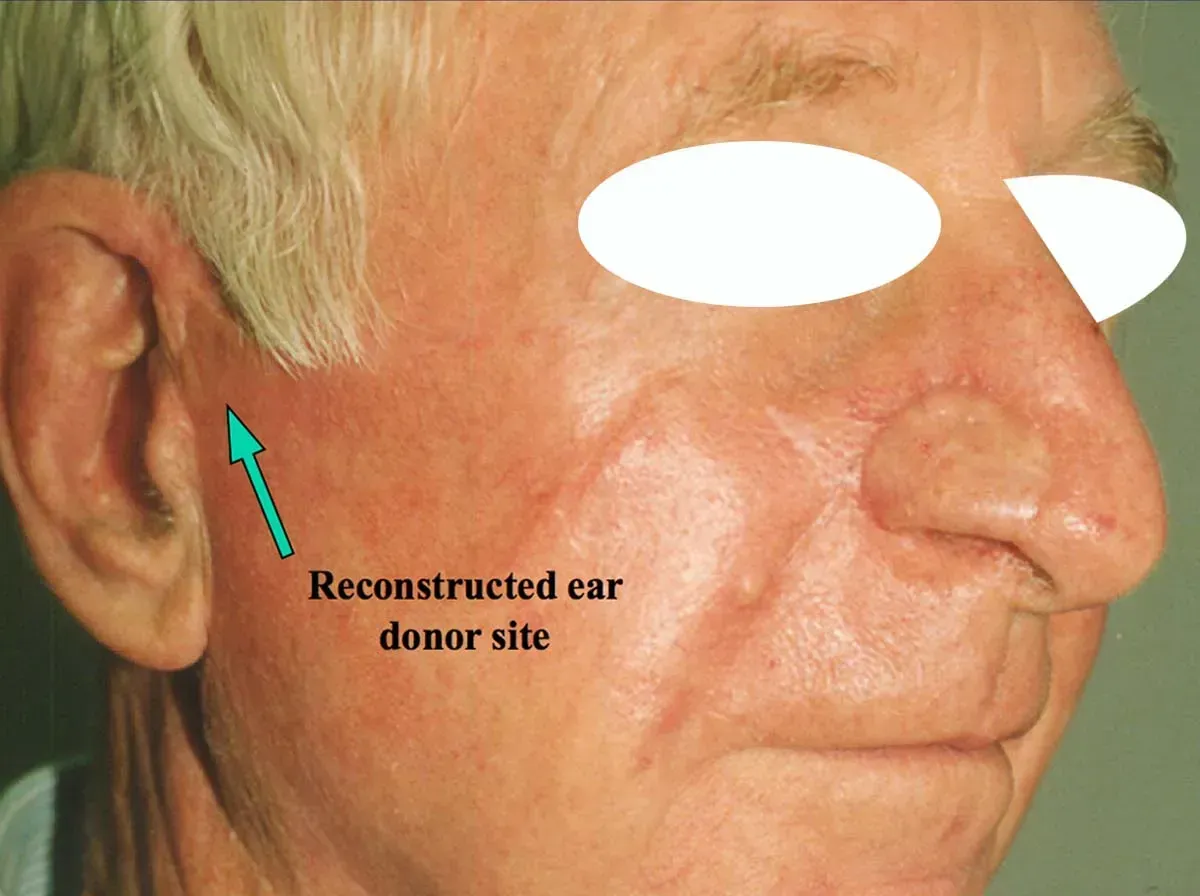
MOHS PROCEDURE NOSE FROM HELL
Why I became expert in MOHS
A dermatologist in Miami, trained by Mohs himself, asked if I would close a patient who lived locally. Sure.
At 3 pm, a male arrived with a full-thickness loss of his right nose! My first introduction to the
MOHS procedure was before modern H & E stains were used. I was now faced with having to provide an inner lining for the
nose, an outer skin, and a cartilage support for the nostril rim! Thinking on your feet is the exciting part of trauma and reconstructive surgery. The problem was defined, now the solution.




BASIC PRINCIPLES AND ENGINEERING
Every injury or lesion is different. There are hundreds of variations that have to be mastered to plan and customize an excision and repair. On the spot improvisation is the name of the game.
LIPOMA MONSTER
My facelift patient came in with a scar down the side of her arm with Frankenstein railroad tracts. I asked if she broke her arm and had surgery. “No”, she said, “I had a lipoma removed by a general surgeon in the next town.” I could not believe the butcher job, and I knew the surgeon was married to a plastic surgeon to make matters worse. The incentive for monster scars is that insurance pays by the length of the wound! I called him and said impolite things.
I then decided to find a better way.



CAN YOU SPOT MY FLAP?
This is a very challenging basal cell carcinoma impinging on the medial canthus and tear duct. A lower lid and cheek rotation flap was engineered without distorting or altering the function of the lower lid. Quite a fun adventure. Can you see the flap? Not to worry, neither can I. 🧐 🕵️♀️ 🔍

